

Jose Manuel Sánchez
Psicologo del Deporte y Fisioterapeuta
Profesor Master de Alto Rendimiento del F.C.Barcelona
www.recuperadoresdeportivos.es
jose@recuperadoresdeportivos.es
RESUMEN :
La tendinopatía rotuliana o “jumper’s knee” se considera más unp proceso degenerativo que nop una “tendinitis inflamatoria” propiamente dicha.Los estudios histopatológicos no muestran presencia de infiltrado de células inflamatorias, si no más bien disrupcionesp de las fibras de colágeno,degeneración mixoide y signos anóxicos de los tenocitos.La Electrólisis Percutánea Intratendinosa (EPI) consiste mediante la aplicación de corriente galvánica de alta intensidad a través dep agujas catódicas provocar una reacción electroquímica en la región delp tendón degenerada.La disociación de las moléculas de agua y sal en sus elementos constitucionales dará lugar porp inestabilidad iónica a la formación de moléculas de hidroxido de sodio (lejía).La “lejía organica”producida debajo del electrodo activo o aguja catódica provocará una respuesta inflamatoria muy localizada sólo y exclusivamente en la región que hemos tratado,permitiendo la fagocitosis y curación del tendón.
MATERIAL Y MÉTODOS.
pSe realiza un análisis de supervivencia mediante el método de Kaplan-Meier dependiendo de la clasificación Victorian Institute of Sport Assessment (VISA) en 34 deportistas con tendinopatía rotuliana que se les aplica Electrólisis Percutánea Intratendinosa.El número total de rodillas tratadas fue de 39 y el rango de edad era de 16 a 53 años (media,25,4 años).De los 34 pacientes ,33 eran diagnosticados de entesopatía del polo inferior de la rótula y sólo 1 caso presentaba entesopatía cuadricipital asociado a entesopatía rotuliana.El rango de evolución clínica era de 4 a 288 semanas (media,19,7 meses) y el tiempo de inactividad deportiva como consecuencia de la tendinopatía marcaba un rango de 0 a 240 semanas (media,12,6 meses).Durante la primera observación se les paso la escala VISA y dependiendo de la puntuación obtenida en los 34 pacientes categorizamos dos grupos: GRUPO 1 (17 pacientes quep durante la primera observación puntuaron con una VISA <50 = Pacientes de peor pronóstico) y GRUPO 2 (17 pacientes que en la primera observación puntuaron con una VISA > 50 = Pacientes de mejor pronóstico).

Fig1: patellar tendon anesthesia


Fig. 3: Sportsman with patellar tendonitis of a year of evolution, A) treatment with PIE in inferior border patellar.B)PIE in medial face of the patellarp tendon (SànchezJM, 2002).
RESULTADOS:de los 17 pacientes del GRUPO 1 o peor pronóstico,7 abandonaron el tratamiento.A la 6ª semana de tratamiento el 50,2% de los pacientes habían curado y a las 8 semanas el 77%.Un 27% de pacientes no se habían curado a las 10 semanas del tratamiento.La media respecto al tiempo empleado para el grupo 1 de pacientes curados fue de 6,8 semanas y la media de sesiones realizadas para la curación fue de 17,4 sesiones.De los 17 pacientes del GRUPO 2 ,15 curaron y 1 abandonó el tratamiento.el porcentaje de pacientes curados fue de 88% y de no curados del 11,7%.La media respecto al tiempo empleado para la curación fue de 2,45 semanas y la media del número de sesiones de 8,7.En la función de supervivencia respecto al tiempo en semanas desde la primera observación a la última para el grupo de peor pronóstico (VISA <50) y el grupo de mejor pronóstico (VISA > 50) existen diferencias estadísticamente significativas (p=0,001).Igualmente en la función de supervivencia respecto al número de sesiones realizadas para el grupo 1 y grupo 2 existen diferencias estadísticamente significativas (p = 0,0006).
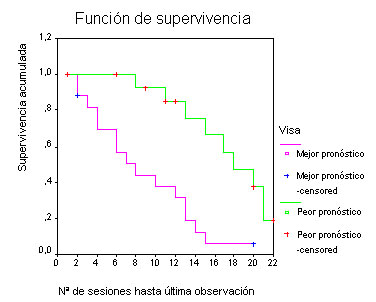
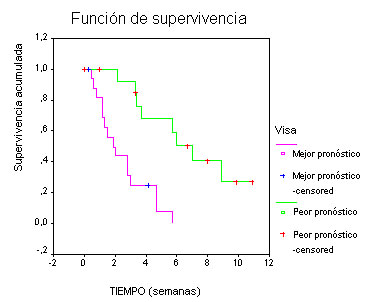
Graph A. Function survival regarding the number of sessions for the group of worse pronostic (VISA <50) and of the group of better pronostic (VISA> 50) being the statistical significance of p = 0,0006.Graph B.. Function survival regarding the time from the first observation to the last observation for the group of worse pronostic (VISA <50) and of the group of better pronostic (VISA> 50) with differences statistically significant being the value p = 0,0001
CONCLUSIONES : Se observa que la técnica de Electrólisis Percutánea Intratendinosa (EPI) es muy eficaz en el tratamiento de las tendinopatías rotulianas , independiente de su tiempo de evolución clínica y clasificación Blazina et al (1972) 28 pacientes estaban en estadio III (82,3%)p y 6 en estadio IIp (17,6%).Los pacientes de mejor pronóstico son los que en la primera observación puntuan con una VISAp > 50,curándose el 100% a las 15 sesiones de tratamiento y con una media de 2,45 semanas.Los pacientes de peor pronóstico son los que puntuan en la primera observación con una VISA < 50.Aun así,un 50% pueden curar en 17 sesiones de tratamiento y en un período de 6 semanas.La escala VISA es un instrumento eficaz para el pronóstico de los pacientes con tendinopatía rotuliana que se les aplica Electrólisis Percutánea Intratendinosa (EPI) independientemente del tiempo de evolución clínica.
Referencias del autor:
Sánchez,JM : Fisiopatología de la regeneración de los tejidos blandos.En Fisioterapia del aparato locomotor.Ed Mc Graw Hill.2005.
Sánchez,JM.Regeneración acelerada de las lesiones musculares en el futbolista profesional.Publicación digital en www.efisioterapia.net,2004.
Sánchez,JM .Tratamiento de la entesopatía rotuliana en deportistas mediantep Microregeneración Endógena Guiada (MEG)Análisis de supervivencia dependiendo de la clasificación Victorian Institute of Sport Assessment (VISA). Memoria de Tesis Doctoral por lap Universitat Internacional Cataluña ,2003.
Sánchez,JM. ¿Fascitis o Fasciosis plantar?.Bases biológicas de su tratamiento mediante electrólisis percutánea intratisular (EPI).Podologia Clinica 5(1)pags.22-29,2004.
Sánchez,JM.Análisis isocinético de los eversores e inversores en la estabilidad dinámica de la zona de inversión del tobillo.Revista de Fisioterapia ,vol.20,monogràfico,p.65-80.Madrid 1998.
Sánchez,JM,Badal L .Complicaciones en la reconstrucción del ligamento cruzado anterior de la rodilla,Divulgación Científica de los Laboratorios Carín,nº5,p.4-6.Barcelona,1997.
Sánchez,JM ,Oregui O,Gonzalez I .Terapia de Neuromodulación Percutánea (TNP) en la evolución del hombro doloroso hiperagudo.En el Third European Congress of Sports Medicine and Science in Tennis.Barcelona,2001.
Sánchez,JM .Dinamometría muscular isocinética.p Revista de Fisioterapia,nº2,1993.
Sánchez,JM.Síndrome de fricción de la bandeleta iliotibial.Tratamiento mediante Electrólisis Percutánea Intratisular (EPI) asociado a microregeneración percutánea. Publicación digital en
www.efisioterapia.net,2004
Sánchez ,JM.Modelos teóricos del dolor en la tendinopatía rotuliana del deportista.Publicación digital en www.efisioterapia.net;2003
Sánchez, JM.Terapia acelerada de la tendinopatía rotuliana del deportista mediante la técnica de Eectrólisis Percutánea Transtendinosa (EPI).Publicación digital en www.efisioterapia.net,2003
Sánchez JM .Bases científicas de la fisioterapia acelerada en la reconstrucción del LCA mediante la técnica de H-T-H.Publicación digital en www.efisioterapia.net,2003.
Referencias básicas
1.Almekinders, LC.,Temple, JD.:Etiology, diagnosis, and treatment of tendonitis: an analysis of the literature. Med Sci Sports Exerc 30, 1183,1998.
2.Almekinders LC., Vellema JH., Weinhold PS.:Strain patterns in the patellar tendon and the implications for patellar tendinopathy. Knee Surg Sports Traumatol Arthrosc.Jan;10(1):2-5. Epub 2001 Aug 16,2002.
3.Blazina, ME., Kerlan, RK., Jobe, FW., Carter, VS.,Carlson, JG.:Jumpers knee. Orthop Clin North Am 4, 665,1973.
4.Bodne D., Quinn SF., Murray WT., Bolton T, Rudd S., Lewis K., Daines P, Bishop J., Cochran C.:Magnetic resonance images of chronic patellar tendinitis. Skeletal Radiol. 17(1):24-8,1988.
5.Bolga, LA., Keskula, DR.:Reliability of lower extremity functional performance tests. J Orthop Sports Phys Ther 26, 138,1997.
6.Bose, K., Kanagasuntheram, R.,Osman, MBH.:Vastus medialis oblique: an anatomical and physiologic study. Orthopedics 3, 880,1980.
7.Carr JC., Hanly S., Griffin J., Gibney R.:Sonography of the patellar tendon and adjacent structures in pediatric and adult patients. AJR Am J Roentgenol.p Jun;176(6):1535-9,2001.
8.Clancy, WG. Leadbetter, WB., Buckwalter, JA., Gordon, SL.: Sports-Induced Inflammation. (American Academy of Orthopaedic Surgeons, Park Ridge, IL),1990.
9.Coleman BD., Khan KM., Kiss ZS, Bartlett J., Young DA., Wark JD.:Open and arthroscopic patellar tenotomy for chronic patellar tendinopathy. A retrospective outcome study. Victorian Institute of Sport Tendon Study Group. Am J Sports Med. Mar-Apr;28(2):183-90,2000.
10.Coleman BD., Khan KM., Maffulli N., Cook JL., Wark JD.:Studies of surgical outcome after patellar tendinopathy: Clinical significance of methodological deficiencies and guidelines for future studies. Victorian Institute of Sport Tendon Study Group. Scand J Med Sci Sports.Feb;10(1):2-11,2000.
11.Colosimo, AJ., Bassett, FH.:Jumpers knee: diagnosis and treatment .Orthop Rev 19, 139,1990.
12.Cook JL., Khan KM., Kiss ZS., Purdam CR., Griffiths L.:Prospective imaging study of asymptomatic patellar tendinopathy in elite junior basketball players. J Ultrasound Med.Jul;19(7):473-9,2000.
13.Cook, JL., Khan, KM., Harcourt, PR., Grant, M., Young, DA., Bonar, SF.:A cross sectional study of 100 athletes with jumpers knee managed conservatively and surgically .Br J Sports Med 31, 332,1997.
14.Cook JL., Khan KM., Harcourt PR., Kiss ZS., Fehrmann MW., Griffiths L., Wark JD.:Patellar tendon ultrasonography in asymptomatic active athletes reveals hypoechoic regions: a study of 320 tendons. Victorian Institute of Sport Tendon Study Group. Clin J Sport Med. Apr;8(2):73-7,1998.
15.Cook JL., Khan KM., Harcourt PR., Grant M., Young DA., Bonar SF.:A cross sectional study of 100 athletes with jumpers knee managed conservatively and surgically. The Victorian Institute of Sport Tendon Study Group. Br J Sports Med. Dec;31(4):332-6,1997.
16.Cook JL., Khan KM.:What is the most appropriate treatment for patellar tendinopathy?. Br J Sports Med.Oct;35(5):291-4,2001.
17.Danova NA., Muir P.:Extracorporeal shock wave therapy for supraspinatus calcifying tendinopathy in two dogs. Vet Rec.Feb 15;152(7):208-9,2003.
18.Dye SF., Campagna-Pinto D., Dye CC., Shifflett S., Eiman T.:Soft-tissue anatomy anterior to the human patella. Bone Joint Surg Am. Jun;85-A(6):1012-7, 2003.
19.Dye SF.:Functional morphologic features of the human knee: an evolutionary perspective. Clin Orthop.May;(410):19-24,2003.
20.Dye SF., Vaupel GL., Dye CC.:Conscious neurosensory mapping of the internal structures of the human knee without intraarticular anesthesia. Am J Sports Med.Nov-Dec;26(6):773-7,1998.
21.Eifert-Mangine, M., Brewster, C., Wong, M., et al.:Patellar tendinitis in the recreational athlete. Orthopedics 15, 1359,1992.
22.Ferretti, A.:Epidemiology of jumpers knee. Sports Med 3, 289,1986.
23.Ferretti, A., Puddu, G., Mariani, PP.,Neri, M.:The natural history of jumpers knee: patellar or quadriceps tendonitis. Int Orthop 8, 239,1985.
24.Ferretti, A., Ippolito, E., Mariani, P., Puddu, G.:Jumpers knee .Am J Sports Med 11, 58,1983.
25.Fyfe I., Stanish WD.: The use of eccentric training and stretching in the treatment and prevention of tendon injuries. Clin Sports Med. Jul;11(3):601-24,1992.
26.Fornage BD., Rifkin MD., Touche DH., Segal PM.: Sonography of the patellar tendon: preliminary observations. AJR Am J Roentgenol.Jul;143(1):179-82,1984.
27.Gerster JC., Landry M, Rappoport G., Rivier G., Duvoisin B., Schnyder P.: Enthesopathy and tendinopathy in gout: computed tomographic assessment. Ann Rheum Dis.Dec;55(12):921-3,1996.
28.Gothelf A., Mir LM., Gehl J.: Electrochemotherapy: results of cancer treatment using enhanced delivery of bleomycin by electroporation. Cancer Treat Rev.p Oct;29(5):371-87,2003.
29.Greene BL.: Physical therapist management of fluoroquinolone-induced Achilles tendinopathy. Phys Ther. Dec;82(12):1224-31,2002.
30.Haake M., Wirth T., Schmitt J.:Focussing of extracorporal shock wave therapy (ESWT) in the treatment of calcifying tendinitis. Joint Bone Spine. May;69 (3) : 344-5,2002.
31.Hayes DW J.r, Gilbertson EK., Mandracchia VJ., Dolphin TF.:Tendon pathology in the foot. The use of corticosteroid injection therapy. Clin Podiatr Med Surg.Oct;17(4):723-35,2000.
32.Hanten, WP., Schulthies, SS.:Exercise effect on electromyographic activity of the vastus medialis oblique and vastus lateralis muscles. Phys Ther 70, 561,1990.
33.Haspl M., Dubravcic-Simunjak S., Bojanic I., Pecina M.:Anterior knee pain associated with sports and work. Arh Hig Rada Toksikol. Dec;52(4):441-9,2001.
34.Haupt G.:Use of extracorporeal shock waves in the treatment of pseudarthrosis tendinopathy and other orthopedic diseases. Urol. Jul;158(1):4-11,1997.
35.Heller R., Coppola D., Pottinger C., Gilbert R., Jaroszeski MJ.: Effect of electrochemotherapy on muscle and skin. Technol Cancer Res Treat. Oct;1(5):385-92,2002.
36.Hess GP., Cappiello W.L, Poole RM., Hunter SC.: Prevention and treatment of overuse tendon injuries. Sports Med.Dec;8(6):371-84,1989.
37.Hodges, PW.,Richardson, CA.:The influence of isometric hip adduction on quadriceps femoris activity. Scand J Rehabil Med 25, 57,1993.
38.Horvath G.: Therapy of injuried Achilles tendon in athletes with balneotherapy in Piestany. Acta Chir Orthop Traumatol Cech. Feb;35(1):86-8,1968.
39.Jakob RP., Segesser B.: Extension training of the quadriceps-a new concept in the therapy of tendinoses of the knee extensor apparatus (jumpers knee). Orthopade. Jun;9(3):201-6,1980.
40.Jaroszeski MJ., Coppola D., Pottinger C., Gilbert RA, Heller R.: Electrochemotherapy for the treatment of human sarcoma in athymic rats. Technol Cancer Res Treat.Oct;1(5):393-9,2002.
41.Jozsa, L.,Kannus, P.:Human Tendons: Anatomy, Physiology, and Pathology. (Human Kinetics, Champaign, IL),1997.
42.Karst, GM., Jewett, PD. :Electromyographic analysis of exercises proposed for differential activation of medial and lateral quadriceps femoris muscle components. Phys Ther 73: 286,1993.
43.Khan, KM., Cook, JL., Bonar, F., Harcourt, P.,Astrom, M.:Histopathology of common tendinopathies: update and implications for clinical management .Sports Med 27, 393,1999.
44.Khan KM., Visentini PJ., Kiss ZS., Desmond PM., Coleman BD., Cook JL., Tress BM., Wark JD., Forster BB.:Correlation of ultrasound and magnetic resonance imaging with clinical outcome after patellar tenotomy: prospective and retrospective studies. Victorian Institute of Sport Tendon Study Group. Clin J Sport Med.Jul;9(3):129-37,1999.
45.Khan KM., Cook JL., Kiss ZS., Visentini PJ., Fehrmann MW., Harcourt PR., Tress BW., Wark JD.: Patellar tendon ultrasonography and jumpers knee in female basketball players: a longitudinal study. Clin J Sport Med. Jul;7(3):199-206,1997.ç
46.Khan KM., Bonar F., Desmond PM., Cook JL., Young DA., Visentini PJ., Fehrmann MW., Kiss ZS., OBrien PA., Harcourt PR., Dowling RJ., .OSullivan RM., Crichton KJ., Tress BM., Wark JD. :Patellar tendinosis (jumpers knee): findings at histopathologic examination, US, and MR imaging. Victorian Institute of Sport Tendon Study Group. Radiology. Sep;200(3):821-7,1996.
47. Khan K; Cook J.:The painful nonruptured tendon: clinical aspects. Clin Sports Med. Oct;22(4):711-25,2003.
48.Kelly, DW., Carter, VS., Jobe, FW.,Kerlan, RK.:Patellar and quadriceps tendon ruptures: jumpers knee. Am J Sports Med 12, 3,1984.
49.Kettunen JA., Kvist M., Alanen E., Kujala UM.: Long-term prognosis for jumpers knee in male athletes. A prospective follow-up study. Am J Sports Med. Sep-Oct;30(5):689-92,2002.
50.Kitamura A.: Bleomycin-mediated electrochemotherapy in mouse NR-S1 carcinoma. Cancer Chemother Pharmacol. Apr;51(4):359-62. Epub 2003 Mar 21,2003.
51.Krahl H.:Jumpers knee"-etiology, differential diagnosis, and therapy. Orthopade.Jun;9(3):193-7,1980.
52.Kujala, UM., Jaakkola, LH., Koskinen, SK., Taimela, S., Hurme, M., Nelimarkka, O.:Scoring of patellofemoral disorders .Arthroscopy 9, 159,1993.
53.Kujala, UM., Osterman, K., Kvist, M., Aalto, T.,Friberg, O.:Factors predisposing to patellar chondroplasty and patellar apicitis in athletes .Int Orthop 10, 195,1986.
54.Kujala UM., Kvist M, Osterman K.:Knee injuries in athletes. Review of exertion injuries and retrospective study of outpatient sports clinic material. Sports Med.p Nov-Dec;3(6):447-60,1986.
55.Kvist M., Jarvinen M.:Clinical, histochemical and biomechanical features in repair of muscle and tendon injuries. Int J Sports Med.Feb;3 Suppl 1:12-4,1982.
56.Laine HR., Harjula A., Peltokallio P.:Ultrasound in the evaluation of the knee and patellar regions. J Ultrasound Med.Jan;6(1):33-6,1987.
57.Laprade, J., Culham, E., Brouwer, B.: Comparison of five isometric exercises in the recruitment of the vastus medialis oblique in persons with and without patellofemoral pain syndrome. J Orthop Sports Phys Ther 27:197,1998.
58.Leadbetter, WB.:Cell-matrix response in tendon injury .Clin Sports Med 11, 533,1992.
59.Lian O., Holen KJ., Engebretsen L., Bahr R.: Relationship between symptoms of jumpers knee and the ultrasound characteristics of the patellar tendon among high level male volleyball players. Scand J Med Sci Sports. Oct;6(5):291-6,1996.
60.Luo QD., Xing ZM., Xiao W., Dai N., Shan YH., Huang GY., Luo SL.: Clinical observations in 185 cases of ligament and tendon injuries treated by the method of dissipating blood stasis and promoting the meridian. Tradit Chin Med. Mar;9(1):15-7,1989.
61.Maddox PA., Garth WP Jr.: Tendinitis of the patellar ligament and quadriceps (jumpers knee) as an initial presentation of hyperparathyroidism. A case report. Bone Joint Surg Am. Feb;68(2):288-92,1986.
62.Magalini, SI.,Magalini, SC.:Dictionary of Medical Syndromes 4th ed .(Lippincott-Raven Publishers, Philadelphia, PA,1997.
63.Marsolais D., Cote CH., Frenette J.: Nonsteroidal anti-inflammatory drug reduces neutrophil and macrophage accumulation but does not improve tendon regeneration. Lab Invest.Jul;83(7):991-9,2003.
64.Martin DF., Carlson CS., Berry J., Reboussin BA., Gordon ES., Smith BP.: Effect of injected versus iontophoretic corticosteroid on the rabbit tendon. South Med J. Jun;92(6):600-8,1999.
65.Min BH., Han MS., Woo JI, Park HJ., Park SR.: The origin of cells that repopulate patellar tendons used for reconstructing anterior cruciate ligaments in man. J Bone Joint Surg Br. Jul;85(5):753-7,2003.
66.Mohtadi, N.: Development and validation of the quality of life outcome measure (questionnaire) for chronic anterior cruciate ligament deficiency .Am J Sports Med 26, 350,1998.
67.Miyazaki S., Gunji Y., Matsubara H., Shimada H., Uesato M., Suzuki T., Kouzu T., Ochiai T.: Possible involvement of antitumor immunity in the eradication of colon 26 induced by low-voltage electrochemotherapy with bleomycin. Surg Today.33(1):39-44,2003.
68.Noyes, FR., McGinniss, GH., Mooar, LA.:Functional disability in the anterior cruciate insufficient knee syndrome: knee rating systems and projected risk factors in determining treatment.Sports Med 1, 278,1984.
69.Orava S., Osterback L., Hurme M.:Surgical treatment of patellar tendon pain in athletes. Br J Sports Med.Dec;20(4):167-9,1986.
70.Orava S., Rantanen J., Kujala UM.: Fasciotomy of the posterior femoral muscle compartment in athletes. Int J Sports Med.Jan;19(1):71-5,1998.
71.Orava S., Kujala UM.: Rupture of the ischial origin of the hamstring muscles. Am J Sports Med.Nov-Dec;23(6):702-5,1995.p
72.Paavola M., Kannus P., Jarvinen TA., Jarvinen TL., Jozsa L., Jarvinen M.: Treatment of tendon disorders. Is there a role for corticosteroid injection?. Foot Ankle Clin.Sep;7(3):501-13,2002.
73.Paavola M., Kannus P., Jarvinen TA., Khan K., Jozsa L., Jarvinen M.: Achilles tendinopathy. J Bone Joint Surg Am.Nov;84-A(11):2062-76,2002.
p 74.Peers KH., Lysens RJ., Brys P., Bellemans.:Cross-sectional outcome analysis of athletes with chronic patellar tendinopathy treated surgically and by extracorporeal shock wave therapy. Clin J Sport Med. Mar;13(2):79-83,2003.
75.Perlick L., Korth O., Wallny T., Wagner U., Hesse A., Schmitt O.: The mechanical effects of shock waves in extracorporeal shock wave treatment of calcific tendinitis--an in vitro model. Z Orthop Ihre Grenzgeb.Jan-Feb;137(1):10-6,1999.
76.Petschnig, R., Baron, R.,Albrecht, M.: The relationship between isokinetic quadriceps strength test and hop tests for distance and one-legged vertical jump test following anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther 28, 23,1998.
77.Pierets K., Verdonk R., De Muynck M., Lagast J.:Jumpers knee: postoperative assessment. A retrospective clinical study. Knee Surg Sports Traumatol. Arthrosc. 7(4):239-42,1999.
78.Popp, JE., Yu, JS.,Kaeding, CC. :Recalcitrant patellar tendinitis: magnetic resonance imaging, histologic evaluation, and surgical treatment .Am J Sports Med 25, 218,1.
79.Puddu G. The effect of volleyball playing on the knee extensor mechanism. Am J Sports Med. 1990 Jan-Feb;18(1):112.
80.Richards DP., Ajemian SV., Wiley JP., Brunet JA., Zernicke RF.: Relation between ankle joint dynamics and patellar tendinopathy in elite volleyball players. Clin J Sport Med.Sep;12(5):266-72,2002.
81.Richards DP., Ajemian SV., Wiley JP., Zernicke RF.: Knee joint dynamics predict patellar tendinitis in elite volleyball players. Am J Sports Med. Sep-Oct;24(5):676-83,1996.
82.Robinson JM., Cook JL., Purdam C., Visentini PJ., Ross J., Maffulli N., Taunton JE., Khan KM.: The VISA-A questionnaire: a valid and reliable index of the clinical severity of Achillestendinopathy. Br J Sports Med. Oct;35(5):335-41,2001.
83.Roels, J., Martens, M., Mulier, JC., Burssens, A.: Patellar tendinitis (jumpers knee). Am J Sports Med 6, 362,1978.
84.Salomskaite-Davalgiene S., Venslauskas MS., Pauziene N.:Histological analysis of electrochemotherapy influence in Lewis lung carcinoma. Medicina (Kaunas).38(5):540-4,2002.
85.Sandmeier R., Renstrom PA.:Diagnosis and treatment of chronic tendon disorders in sports. Scand J Med Sci Sports. Apr;7(2):96-106,1997.
86.Sanchis-Alfonso V., Rosello-Sastre E., Subias-Lopez A.:Neuroanatomic basis for pain in patellar tendinosis ("jumpers knee"): a neuroimmunohistochemical study. Am J Knee Surg. Summer;14(3):174-7,2001.
87.Sanchis-Alfonso V., Rosello-Sastre E.:Immunohistochemical analysis for neural markers of the lateral retinaculum in patients with isolated symptomatic patellofemoral malalignment. A neuroanatomic basis for anterior knee pain in the active young patient. Am J Sports Med.Sep-Oct;28(5):725-31,2000.
88.Sanchis-Alfonso V., Rosello-Sastre E., Monteagudo-Castro C., Esquerdo J.:Quantitative analysis of nerve changes in the lateral retinaculum in patients with isolated symptomatic patellofemoral malalignment. A preliminary study. Am J Sports Med. Sep-Oct;26(5):703-9,1998.
89.Sanchis-Alfonso V., Subias-Lopez A., Monteagudo-Castro C., Rosello-Sastre E.:Healing of the patellar tendon donor defect created after central-third patellar tendon autograft harvest. A long-term histological evaluation in the lamb model. Knee Surg Sports Traumatol Arthrosc.7(6):340-8,1997.
90.Scranton, PE.,Farrar, EL.:Mucoid degeneration of the patellar ligament in athletes .J Bone Joint Surg Am 74, 435,1992.
91.Seil R., Rupp S., Hammer DS., Ensslin S., Gebhardt T., Kohn D.: Extracorporeal shockwave therapy in tendionosis calcarea of the rotator cuff: comparison of different treatment protocols. Orthop Ihre Grenzgeb.Jul-Aug;137(4):310-5,1999.
92.Schmid MR., Hodler J., Cathrein P., Duewell S., Jacob HA., Romero J.:Is impingement the cause of jumpers knee? Dynamic and static magnetic resonance imaging of patellar tendinitis in an open-configuration system. Am J Sports Med.May-Jun;30(3):388-95,2002.
93.Shimizu T., Nikaido T., Gomyo H., Yoshimura Y., Horiuchi A., Isobe K., Ebara S., Takaoka K.:Electrochemotherapy for digital chondrosarcoma. J Orthop Sci. ;8(2):248-51,2003.
94.Stanish, WD., Rubinovich, RM.,Curwin, S.: Eccentric exercise in chronic tendinitis. Clin Orthop 208, 65,1986.
95.Stanish WD., Curwin S., Rubinovich M.:Tendinitis: the analysis and treatment for running. Clin Sports Med.Oct;4(4):593-609,1985.
96.Tarsney FF.:Catastrophic jumpers knee. A case report. Am J Sports Med. Jan-Feb;9(1):60-1,1981.
97.Wang LQ., Wang AM., Zhang SD.: Clinical analysis and experimental observation on acupuncture and moxibustion treatment of patellar tendon terminal disease in athletes. J Tradit Chin Med.Sep;5(3):162-6,1985.
98.Wojtys EM., Beaman DN., Glover RA., Janda D.:Innervation of the human knee joint by substance-P fibers. Arthroscopy. 6(4):254-63,1990.
99.Zakaria, D., Harburn, KL., Kramer, JF.:Preferential activation of the vastus medialis oblique, vastus lateralis, and hip adductor muscles during isometric exercises in females. J Orthop Sports Phys Ther 26, 23,1997.
100.Zarins B., Ciullo JV.: Acute muscle and tendon injuries in athletes. Clin Sports Med.Mar;2(1):167-82,1983.